
Once again, COVID-19 reveals child welfare’s double standards
Are you a parent who just can’t handle the demands of your own work, the stress of coronavirus and educating your child from home while schools are closed?
If you’re middle-class you can get indulgence, sympathy and helpful hints. Your kids can “play Fortnite for the next eight hours.”
If you’re poor you can get a caseworker at the door investigating you for “educational neglect.”
by Richard Wexler
National Coalition for Child Protection Reform
Excerpts:
All over America, parents are finding out just how hard it is to be a teacher – particularly when it’s your own child and everyone has to master new technology and new lessons at the same time.
The New York Times feels your pain. In a story filled with examples of middle-class parents struggling to cope – or even giving up – the story declares:
With teachers relegated to computer screens, parents have to play teacher’s aide, hall monitor, counselor and cafeteria worker — all while trying to do their own jobs under extraordinary circumstances. …
Kindergartners need help logging into Zoom. Seventh-graders need help with algebra, last used by dad circa 1992. “School” often ends by lunchtime, leaving parents from Long Island to Dallas to Los Angeles asking themselves the same question: How bad am I if my child plays Fortnite for the next eight hours?
If you’re middle class, not bad at all. In fact, you can give up entirely! Again, from the story:
The litmus tweet of the moment came from Sarah Parcak, an archaeologist at the University of Alabama at Birmingham.
“I told our son’s (lovely, kind, caring) teacher that, no, we will not be participating in her ‘virtual classroom,’ and that he was done with the 1st grade,” she wrote on Twitter in early April. “We cannot cope with this insanity. Survival and protecting his well being come first.”
Yes, that’s right – if you’re white and middle class you can announce to the whole world that your child is “done with first grade” and not have to worry. It’s similar to how middle-class moms can brag about using marijuana.
To the surprise of, I’m guessing, pretty much no one, whether its pot or education, it doesn’t work that way if you’re poor.
If you’re poor, it’s “educational neglect”
Shortly after New York City schools closed, I started hearing rumors that schools were actually calling in “educational neglect” reports on parents when their kids didn’t “show up for class” online – because, after all, every child living in poverty has immediate access to all the necessary technology, right?
And what could be better for kids and families in this time of stress than a caseworker from the city’s Administration for Children’s Services caseworker showing up at the door?
Thanks to some good reporting from Eileen Grench at the online news site The City, now we know: The rumors were true. From Grench’s story:
Joyce McMillan, family advocate at Sinergia and founder of the Parent Legislative Action Network, says mothers she works with in homeless shelters have been threatened by children’s school staff with a call to the child neglect hotline — even as they struggled to get diapers, much less share internet limited shelter hotspots.
“If we know this is the population of people that we’re working with,” asked McMillan, “why are you using informants if you know [families] can’t comply?”
The city’s Department of Education (DOE) says teachers and others are supposed to check first to see if the problem is lack of technology. But teachers are mandated reporters – subject to severe penalties if they don’t report. So it’s easier – for them – to just call in the report.
All this is on top of the fact that there is abundant evidence that “educational neglect” is so useless when it comes to finding actual child abuse, so harmful to children, families and to education, and so easily abused, that it probably should not even be something that can be reported to child protective services at all.
Read the full article at the National Coalition for Child Protection Reform.
Comment on this article at MedicalKidnap.com.
by GMWatch.org
Excerpts:
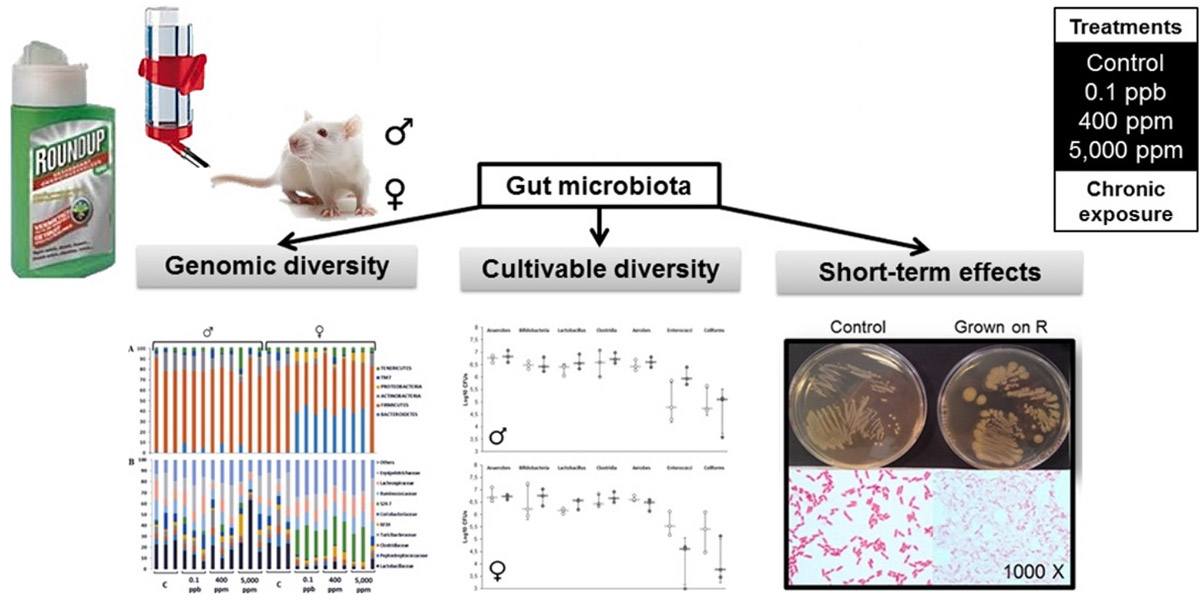
An environmentally relevant concentration of Roundup caused changes in the gut microbiome of rats, according to a new study published by the group of Prof Gilles-Eric Séralini at the University of Caen, France.
Our analysis of the study (see abstract below) and its findings follows.
Study design
Analyses were carried out of the faecal samples from rats used in the long-term Seralini study. The faeces from 3 animals per Roundup treatment group were analysed for gut microbiome.
In addition, bacteria were grown in vitro from the faeces of control animals and treated with increasing concentrations of Roundup.
Main findings
The main findings were a sex-specific alteration in the gut microbiome of female rats only, tested in vivo. Specifically, there was an increase in the Bacteroidetes family S24-7 and a decrease in the Lactobacillacea family of bacteria.
The same gut microbiome alterations were observed in vivo at all of the three doses of Roundup administered. Thus there was no dose-response effect (in which the effect changes with dose).
Bacteria grown in vitro from the faeces of control animals and treated with increasing concentrations of Roundup showed growth inhibition. This demonstrated a direct growth inhibitory effect of Roundup, but only at high concentrations that far exceeded the doses that the female rats were exposed to in the in vivo experiment.
Limitations
One limitation of the study was that faeces from only three animals per test group of 10 from the long-term study were analyzed – a small sample.
Comments
A possible interpretation of the results is that there is a direct effect of Roundup on the gut microbiome. The authors offer extensive arguments supporting this interpretation. However, some counter-arguments cast doubt on it – notably, that there were no differences in effect between the different doses. Building on this fact, it is known from other studies that surfactants such as those present in glyphosate herbicide formulations (e.g. Roundup) have profound effects on the gut microbiome. Thus increasing doses of Roundup would be expected to result in a more pronounced alteration in gut microbiome. Yet this linear dose response (in which effect increases with dose) was not seen in this study. The in vitro experiments show gut bacterial growth inhibition only at high concentrations.
The authors suggest that gut microbiome “resilience” (that is, adaptation to external disruptive agents) may account for this lack of a dose response to increasing dose of Roundup.
However, there are two points worth taking into account that can provide a more consistent and coherent explantation for the lack of a dose response to Roundup exposure.
First, in vitro experiments in this study show gut bacterial growth inhibition only at high concentrations, suggesting that the alterations in the gut microbiome in vivo may be an indirect rather a direct effect of the Roundup.
Second, the authors acknowledge that it is well documented that functional disturbances in organs distant from the gut, especially the liver, are often associated with marked changes in the gut microbiome. It has been demonstrated that even the lowest dose Roundup treatment group in this study suffered from marked liver structural and functional damage reflective of non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatosis (NASH). The lowest dose of Roundup produced as profound a liver dysfunction as the highest dose. In other words, with regard to the liver damage, the researchers did not see a linear dose response.
Similarly, and as we have seen, the alterations in the gut microbiome observed in these same female rats do not follow a linear dose response. Thus it is quite plausible that they are a result of the liver dysfunction.
This provides the most coherent explanation for the findings of alterations in the gut microbiome.
Read the full article at GMWatch.org
Reference
Sex-dependent impact of Roundup on the rat gut microbiome
Veronica L. Lozano, f, Nicolas Defarge, e, Louis-Marie Rocque, c, Robin Mesnage, d, Didier Hennequin, Renaud Cassier, Joël Spiroux de Vendômois, Jean-Michel Panoff, Gilles-Eric Séralini
Toxicology Reports, Volume 5, 2018, Pages 96–107
https://www.sciencedirect.com/science/article/pii/S2214750017301129

by Christina England
Health Impact News
In 2016, we published an article on the dangers of the meningitis B vaccination, Bexsero, titled, Are Ineffective New Meningitis B Vaccines Causing Harm to Children?
At the time of publication, according to the FDA product information leaflet, the vaccine had in fact only been approved for children over the age of ten.
Despite, this fact however, in the UK, the meningitis B vaccine Bexsero was being administered to infants as young as 2 months, despite the fact that we could find no evidence to support that this vaccine was safe to be administered to babies.
In our previous article, we stated that:
“In the UK, Bexsero is the main vaccination being recommended for babies between the ages of two and six months, a vaccine that, according to the manufacturers vaccine insert, has only been approved for individuals from the ages of 10 through to 25.”
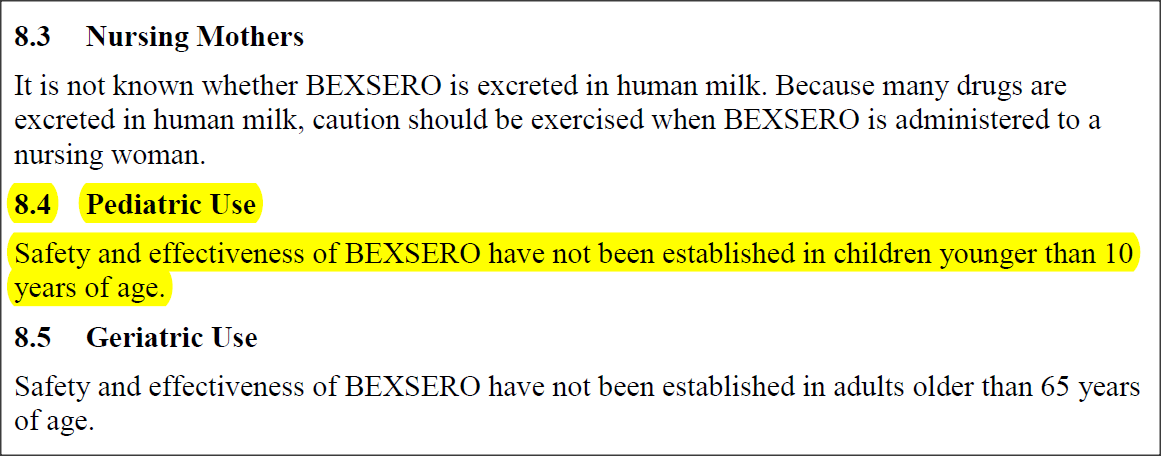
To support our argument, we published the following screenshot from the FDA website:

We continued that:
“What is even more alarming is the fact that the manufacturer has stated that the safety and effectiveness of this vaccine have not been established in children under 10 years of age.”
Once again, to prove that this was the information being provided by the FDA, we published the following screenshot:
In fact, the Centers for Disease Control and Prevention (CDC), now provide similar information to the FDA. In 2016, they stated:
“Serogroup B Meningococcal Vaccines:
Two serogroup B meningococcal vaccines — Bexsero® and Trumenba® — have been licensed by the Food and Drug Administration (FDA).
These vaccines are recommended routinely for people 10 years or older who are at increased risk for serogroup B meningococcal infections, including:
- People at risk because of a serogroup B meningococcal disease outbreak
- Anyone whose spleen is damaged or has been removed
- Anyone with a rare immune system condition called “persistent complement component deficiency”
- Anyone taking a drug called eculizumab (also called Soliris®)
- Microbiologists who routinely work with isolates of N. meningitidis
These vaccines may also be given to anyone 16 through 23 years old to provide short term protection against most strains of serogroup B meningococcal disease; 16 through 18 years are the preferred ages for vaccination.”
Since publishing the article, it has been brought to our attention that there are in fact two product information leaflets on the same vaccination.
However, what is different about the second product information leaflet, published on January 14, 2015, by the European Medical Agency (EMA) is that the information that it provides, is the polar opposite, of the information provided by the FDA.
Who is Correct Regarding the Safety of this Vaccine for Children: The FDA or The EMA?
Due to the fact that the information provided by both agencies is conflicting, how are parents supposed to know which agency is providing the correct information?
For example, in contrast to the FDA, the EMA has confirmed that not only is Bexsero safe and effective, but that it should be given to all babies from the age of eight weeks.
They stated that:
“The first dose should be given at 2 months of age. The safety and efficacy of Bexsero in infants less than 8 weeks of age has not yet been established. No data are available.
In case of delay, the booster should not be given later than 24 months.”
Whereas, the FDA clearly stated that the safety and effectiveness of Bexsero had not been established in children under the age of 10 years, the EMA has stated the complete opposite:
“The safety of Bexsero was evaluated in 14 studies including 10 randomised controlled clinical trials with 8776 subjects (from 2 months of age) who received at least one dose of Bexsero. Among Bexsero recipients, 5849 were infants and children (less than 2 years of age), 250 were children (2 to 10 years of age) and 2677 were adolescents and adults. Of the subjects who received primary infant series of Bexsero, 3285 received a booster dose in the second year of life. Data for a further 207 children exposed to Bexsero in a subsequent study have additionally been evaluated.”
The EMA continued:
“In infants and children (less than 2 years of age) the most common local and systemic adverse reactions observed in clinical trials were tenderness and erythema at the injection site, fever and irritability.
In clinical studies in infants vaccinated at 2, 4 and 6 months of age, fever (≥ 38°C) was reported by 69% to 79% of subjects when Bexsero was co-administered with routine vaccines (containing the following antigens: pneumococcal 7-valent conjugate, diphtheria, tetanus, acellular pertussis, hepatitis B, inactivated poliomyelitis and Haemophilus influenzae type b) compared with 44% to 59% of subjects receiving the routine vaccines alone. Higher rates of antipyretic use were also reported for infants vaccinated with Bexsero and routine vaccines. When Bexsero was given alone, the frequency of fever was similar to that associated with routine infant vaccines administered during clinical trials.
When fever occurred, it generally followed a predictable pattern, with the majority resolving by the day after vaccination.
In adolescents and adults, the most common local and systemic adverse reactions observed were pain at the injection site, malaise and headache.”
Confused by the conflicting information being offered to parents, Health Impact News turned to the manufacturer of the vaccine, GlaxoSmithKline, for guidance.
Once again their information published on the GlaxoSmithKline website, July 2017, mirrored information published by the FDA. They stated:
“BEXSERO is a vaccine indicated for active immunization to prevent invasive disease caused by Neisseria meningitidis serogroup B. BEXSERO is approved for use in individuals 10 through 25 years of age.
Approval of BEXSERO is based on demonstration of immune response, as measured by serum bactericidal activity against three serogroup B strains representative of prevalent strains in the United States. The effectiveness of BEXSERO against diverse serogroup B strains has not been confirmed.”
As you can clearly see, the information that is being provided by GlaxoSmithKline, is exactly the same as the information being provided by the FDA.
This being the case, we must ask:
Is the UK government conducting clinical trials on infants, and if they are, then are parents aware of this fact?
All the information that we have discovered during our investigation has indicated that the meningitis B vaccine Bexsero should only be given to children aged 10 – 25 years. Other than the EMA, no agency has provided alternate information.
In a final attempt to find any other alternative view on this we turned to the Joint Committee for Vaccination and Immunization (JCVI).
JCVI Recommend Paracetamol as Bexsero Can Cause an Increased Risk of Fever
The JCVI are an organization that advises the UK health departments on immunization. In 2014, they published a paper titled, JCVI position statement on use of Bexsero® meningococcal B vaccine in the UK.
They wrote:
“This statement sets out the conclusions of the JCVI regarding its deliberations on the cost-effectiveness of using serogroup B meningococcal (MenB) vaccine in the UK, both routinely in infants and/or adolescents and in at risk groups. This statement follows extensive discussion, which the Committee believes was necessary to ensure the most robust conclusion possible was reached. The Committee is of the opinion that its deliberations have
taken into account the views and comments received, and are based on the most up to date and complete scientific evidence on MenB disease and the MenB vaccine Bexsero®. The health economic analyses undertaken comply with the methodology of National Institute of Health and Care Excellence (NICE) and appropriate NICE guidance.” (own emphasis)
Sadly, their evidence appeared to be more about whether or not the vaccine was cost effective, than whether the vaccine was actually safe or not.
However, they did state that:
“JCVI considered safety data from clinical trials totalling over 6000 participants, and reviewed the European Medicines Agency’s (EMA) considerations of this data. As with any new vaccine or medicine, knowledge of the safety profile of the vaccine is limited to the size of the clinical trials, however the Committee in October 2013 agreed these trials suggested there would be benefits to the vaccinated population.”
Although, they continued their statement with the following extremely worrying piece of information:
“Data from clinical trials suggest that the frequency of fever following routine infant immunisations would be expected to substantially increase if Bexsero® was given with other routine infant immunisations however, concomitant administration of prophylactic paracetamol reduced fever rates without significantly reducing immunogenicity, in contrast to a study of concomitant paracetamol with routine infant immunisations (excluding Bexsero®). Data were too limited to identify rare adverse reactions to the vaccine, however the Committee agreed that the infrastructure and expertise available in the UK would allow the acceptability and safety of the vaccine to be assessed.” (own emphasis)
And if this statement was not alarming enough, they continued by adding that:
“JCVI noted evidence of an increased risk of fever when Bexsero® was administered with other childhood immunisations in the UK schedule. Given this, and concerns of the Committee that this could lead to an increase in fever requiring medical attention, or lead to lower uptake of subsequent vaccinations it was agreed there would be a need to educate parents, and healthcare professionals on the potential reactogenicity of provision of Bexsero® concomitantly with other infant vaccinations. Good communications would reduce the impact of fever on the health service, and provision of prophylactic paracetamol at the time or shortly after vaccination, with a further two doses every four to six hours thereafter should reduce the likelihood or intensity of fever, without diminishing the immune response.” (own emphasis)
In other words, the JCVI recognize the fact that this vaccination has the potential to cause a fever severe enough to warrant medical attention, but it is OK because parents can be educated to give their children regular doses of paracetamol, which incidentally, according to the National Health Service, can cause liver failure.
Learn more about the dangers of paracetamol (acetaminophen).
Interestingly, it appears that the chairman of the JCVI, which is the British equivalent of the ACIP (Advisory Committee on Immunization Practices), Prof Andrew J Pollard helped in the manufactuting of Bexsero.
This was reported by Age of Autism who wrote:
“Prof Andrew J Pollard spoke this September at an event sponsored by vaccine manufacturer GlaxoSmithKline “Evening of Evidence/Vaccination Science to Policy: Introduction of new vaccines to the UK vaccine schedule with limited evidence of efficacy (sic): Meningococcal Group B and maternal pertussis vaccination“.
Prof Pollard spoke on the subject of Meningitis B vaccine which he helped to develop and latterly seems to have superintended the process of having it added to the United Kingdom vaccine schedule as chairman of the JCVI – his talk was entitled: “JCVI decision-making process informing the recommendation for the introduction of Bexsero to the UK vaccination schedule”.
Bexsero vaccine was developed by Novartis but their vaccine division was acquired by GSK earlier this year, following the approval of Bexsero vaccine by the JCVI (negotiations began within days of the JCVI approval).
A deputy chair of the JCVI, Dr Andrew Riordan, spoke at the same meeting on the subject: “Evidence considered by the JCVI to recommend antenatal pertussis vaccination in the UK”. GSK also manufacture Boostrix – in fact a pertussis, tetanus and diphtheria vaccine – which is the product currently given to pregnant women in the UK, which also has an aluminium adjuvant.”
With this information in mind, Health Impact News would like to know what is really behind the UK’s decision to give this vaccination to infants as young as eight weeks of age, and should parents be warned that it has not been approved for children under the age of 10 years old?
Comment on this article at VaccineImpact.com.
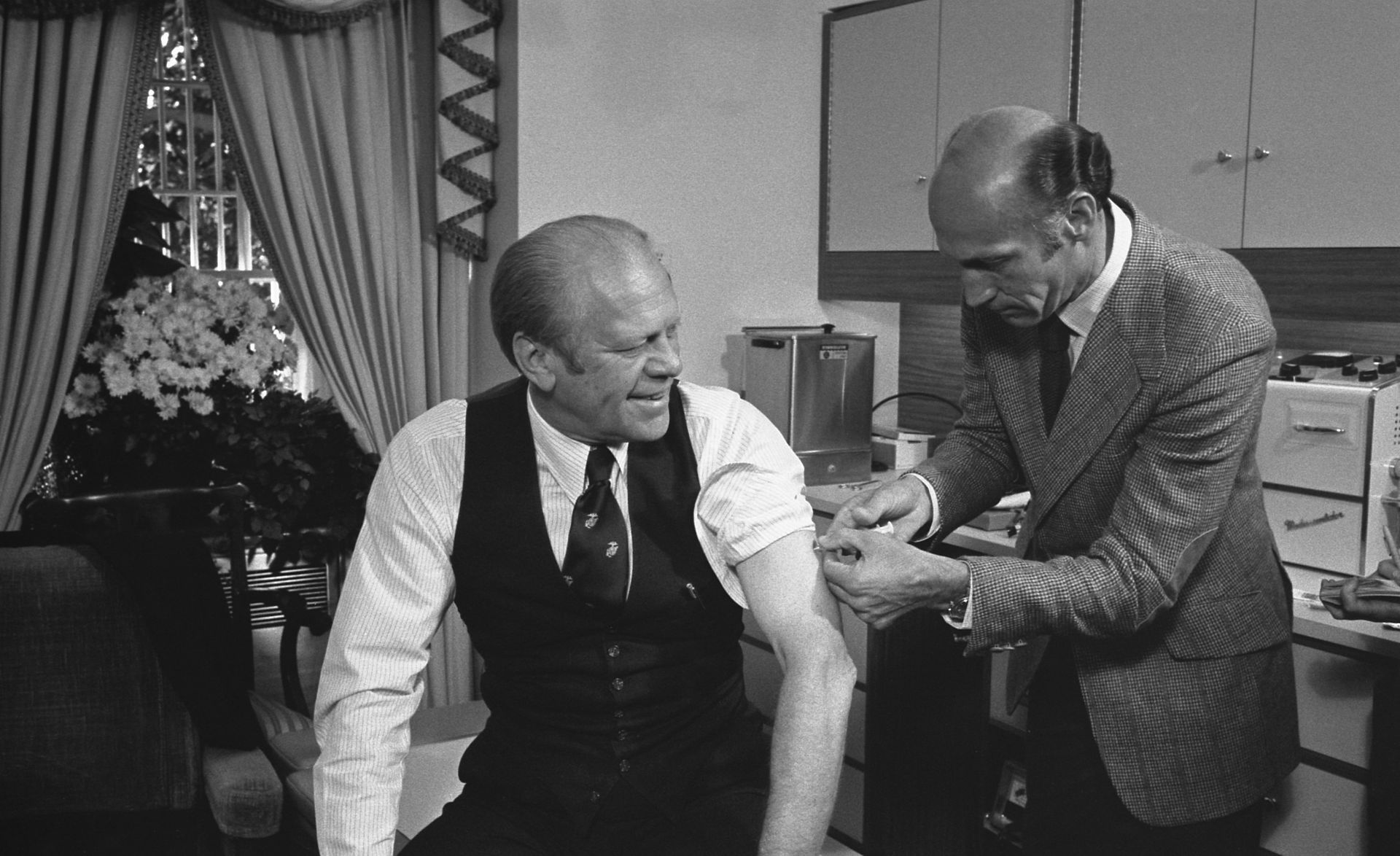
The pharmaceutical industry convinced President Gerald Ford to give them legal immunity from the Swine Flu vaccine which was rushed to market in 1976, and to lead the PR campaign to convince Americans to get the vaccine. More people died from the vaccine than from the flu.
Read this before you consider purchasing a hazmat suit to protect yourself from Ebola!
By John P. Thomas
Health Impact News
Are we facing an Ebola pandemic that will kill millions, or is this just a marketing plan of the pharmaceutical industry to sell more drugs and vaccines? Is the current strain of the Ebola virus a secret creation of pharmaceutical company scientists, biological warfare researchers, or the fruit of Monsanto’s product development team?
Was Ebola created, or did it just accidentally spill over into humans from an animal host such as African fruit bats?
Is the US government intentionally not taking strong action to prevent Ebola from spreading or is there really minimal risk to Americans? Are there groups that want to decrease the world population through spreading contagious diseases such as Ebola, or is this just another imaginary plan that is being reported by certain conspiracy theory groups?
Is the Ebola virus a local epidemic, a global pandemic, or a hoax? Is life in America as we have known it about to collapse into chaos and martial law, or will we be safe and secure once we take the Ebola vaccine?
Will more people die from the Ebola vaccine than would have died from the disease itself?
All these questions have been circulating through the media over the last few months. The situation with Ebola is certainly a complex muddle of contradictory facts, opposing interpretations, and political intrigue. It reminds me very much of the 1976 Swine flu hoax — commonly called the swine flu fiasco or the swine flu debacle.
The Relationship between the 1976 Swine Flu Hoax and Ebola Zaire
To better interpret what is happening with the current Ebola situation, it will be helpful to look at one of the great American examples of health policy gone awry.
For those who don’t remember the 1976 swine flu threat or weren’t living in that era of history, it will be useful to compare the past events to our current situation with Ebola.
In 1976, I was a junior in college. A friend convinced me that I should be concerned about the swine flu that was predicted to devastate the US population. Millions of people were expected to die unless we all lined up and took the flu shot. Reluctantly I gave in to my friends fear and we went and got the vaccine.
Four years later, when I was a public health graduate student, we were required to read a book about the 1976 swine flu hoax. I was shocked by what I read. I was so naive! As a 23 year old graduate student, I found it hard to believe that the system failed so badly. At that time, I truly believed that government officials, physicians, scientists, pharmaceutical companies, and of course public health agencies were all working to promote the health of Americans.
It was disturbing and shocking to learn that faulty scientific interpretations, partisan political interests, opportunities for corporate profit, and personal pride and desire for career advancement were the powerful driving forces behind the development of the 1976 swine flu program.
The whole thing began in February 1976 when an Army recruit at Fort Dix, New Jersey, fell ill and died from a swine flu virus thought to be similar to the 1918 strain, which killed an estimated 500,000 Americans. Based on a relative similarity with the 1918 swine flu, it was determined that millions might soon die unless the US government mobilized a powerful response to protect Americans. It was time to pull out all the stops and show how the public health system could effectively prevent a disaster.
During the spring and summer of 1976, pharmaceutical companies went to work making and stockpiling millions of doses of swine flu vaccine. Then the government went to work inducing sufficient fear among Americans to motivate us to roll up our sleeves and take the shot. We saw pictures of President Gerald Ford receiving his shot, and many of us did the same patriotic deed in the year of our nation’s bicentennial birthday. Taking the vaccine was in many ways advertised as an act of patriotism as well as an act of self-preservation.
Well, in retrospect, the swine flu epidemic of 1976 never developed. It wasn’t because 40 million Americans took the shot. It was because the swine flu never existed. It was nothing more than poor science, flawed judgments and wishful thinking. In short we all were part of a grand hoax.
After all the hype, and only one death and 13 cases of the swine flu, [1] the vaccination program was abruptly cancelled after 10 weeks.
The vaccine program was discontinued on December 16, 1976, because of severe adverse reactions. More than 500 people are thought to have developed Guillain-Barre syndrome after receiving the vaccine, and 25 died from the unexpected adverse reaction. [2, 3]
Guillain-Barre syndrome is a neurological condition which causes temporary paralysis that can lead to death. More people died from the flu vaccine than died from the flu.
Could Ebola be another Grand Hoax in the Making?
At this point I don’t think we can be sure the threat is real. Why would I say such a thing when we know that thousands have died in Africa from the Ebola virus?
This is what the World Health Organization (WHO) has to say about the deaths from Ebola. Please take note of the words that I emphasized with bold type. The report dated October 8, 2014 states:
The total number of confirmed, probable, and suspected cases … in the West African epidemic of Ebola virus disease reported up to the end of October 5, 2014 … is 8033 with 3865 deaths. Countries affected are Guinea, Liberia, Nigeria, Senegal, Sierra Leone, and the United States of America [1 man who travelled from Africa to Texas recently died from Ebola]. A confirmed case of Ebola has been reported in Spain. [4]
I highlighted the words “confirmed, probable, and suspected” in the preceding paragraph, because the number of affected persons and the number of deaths are not all based on scientific testing. The truth is that the WHO numbers simply represent a belief about Ebola incidence and fatalities. People are constantly getting sick and dying in Africa just as they are in the US. In the current situation, where Ebola is likely on the minds of every doctor and nurse in western Africa, it is natural to attribute deaths to Ebola.
Having been part of the public health system as a young person, it is clear to me that we make assumptions, even though our training cautioned us against such behavior. Just as generals in the military can’t wait for the next war so that they can go to work doing what they have spent a lifetime studying — leaders of the public health system, such as those in the World Health Organization, are eager to grab at any opportunity to find a disease threat and to eradicate it. After all, that is their job. Generals and public health officials both think in terms of the next battle to be fought. That is what they will do even when the threat is minimal or maybe does not actually exist. Are the generals of pandemic warfare at the World Health Organization making inferences and assumptions, which might just prove to be wrong?
Is Ebola Testing Accurate?
I read a series of investigate reports from Jon Rappoport which presented stunning evidence that the standard Ebola tests are anything but accurate. He quotes from a Department of Defense manual and explains the instructions concerning Ebola diagnosis. His report states:
The standard test for diagnosing Ebola is the PCR, which has many flaws that render it misleading and useless.
Therefore, “diagnosed with Ebola,” through the PCR test, means nothing. “Ebola” could be flu, could be “drinking contaminated water,” could be any number of non-Ebola conditions.
So when the authorities report there are 6000 cases of Ebola and 3000 deaths, or when they report that two patients in the US have Ebola, they’re relying on a diagnostic test that can’t confirm any of these assertions is true.
This is verified in spades by a Department of Defense manual.
The title is: “Ebola Zaire (EZ1) rRT-PCR (TaqMan®) Assay on ABI 7500 Fast Dx, LightCycler, & JBAIDS: INSTRUCTION BOOKLET” published by “Joint Project Manager Medical Countermeasures Systems.” It is dated 14 August 2014.
Under the title is the statement: “Manufactured by the Naval Medical Research Center for the US DOD.”
Here is a quote [from the Department of Defense manual]:
“[The PCR test] should not be used as the sole basis for patient management decisions. Results [of the PCR] are for the presumptive identification of the Ebola Zaire virus (detected in the West Africa outbreak in 2014).”
Translation: “The word ‘presumptive’ means ‘we’re not sure’. And that’s right. We’re not sure. Don’t rely on the PCR for a definitive diagnosis of Ebola.”
Here is the final quote:
“The definitive identification of the Ebola Zaire virus (detected in the West Africa outbreak in 2014) requires additional testing and confirmation procedures in consultation with public health or other authorities for whom reporting is required. The diagnosis of Ebola Zaire virus (detected in the West Africa outbreak in 2014) infection must be made based on history, signs, symptoms, exposure likelihood, and other laboratory evidence in addition to the identification of the Ebola Zaire virus (detected in the West Africa outbreak in 2014) by this [PCR] test.”
That’s the capper. It baldly states that other diagnostic tests must be run. I can tell you what those other tests should be. One, purification and direct isolation of the virus from the patient; and two, a test to determine the amount of virus in the patient—because millions and millions of active Ebola virus must be present in the patient to even begin to say he is “an Ebola case.” [5]
Do the preceding comments from Jon Rappoport disturb you? Maybe there aren’t as many true cases of Ebola as are being reported. The WHO wants us to believe there is an out of control epidemic in Africa, and they are reporting that their numbers are far below the actual cases of Ebola. We are told that African health officials are so overwhelmed that they can’t even count or report all the Ebola cases. [6]
Jon Rappoport finished his post with this statement:
Press reports are mentioning the fact that far fewer “Ebola patients” than expected are showing blood hemorrhaging. Another tip-off that the PCR test is bringing into the fold “presumptive cases of Ebola”—people who are suffering from factors that have nothing to do with Ebola. [7, 8]
Are other Diseases being Confused with Ebola?
There might be any number of diseases or health conditions that may have symptoms similar to Ebola virus disease. Acute pesticide exposure, acute chemical exposure from an unknown source, or just a common variety of flu could all be confused with true cases of Ebola. If health workers are as overwhelmed as has been reported, then confusion is likely.
An example of this confusion is provided by Jon Rappoport in another article. He states:
Take this example—a farming village in Liberia, one of the so-called epicenters of Ebola. The families manage to produce enough to get by. They live downstream from a giant Firestone rubber plantation.
For years, to no avail, the people of the village have been protesting the runoff of noxious elements into their water supply. Fish are dying. Crops are failing. That means malnutrition, hunger. That means chemical assault on their immune systems.
People are developing sores, lesions, fevers, respiratory problems, digestive problems, including diarrhea.
How easy is it to call this Ebola, in light of the current hysteria? [9]

U.S. military arrived in Liberia Africa in September in response to the “Ebola crisis.” Photo by U.S. Embassy, Liberia
Is it Coincidence that the “Epidemic” and the Vaccine are Arriving Together?
I must wonder how it is that the Ebola vaccine is almost ready for distribution at the same time that we are being told to brace ourselves, because the Ebola virus is on the verge of becoming a worldwide pandemic that could kill millions of us. Here are a few facts that you might find of interest concerning this coincidence.
Major grants have been given by the US military to develop Ebola drugs for the treatment of people who might be exposed to Ebola. In 2006, Alnylam Pharmaceuticals Inc. was reported to gain $23 million over the next four years from an anti-terror drug development contract from the US Defense Department. [10] In 2010, Tekmira was awarded up to 140 million dollars to develop a drug that would prevent Ebola from being turned into a bioterrorism weapon. [11] (See also: U.S. Military Starts Producing Vaccines: New Billion Dollar Experimental Vaccine Market? and The Pentagon’s Vaccine Factories.)
Monsanto has now partnered with the Department of Defense to use a proxy third party company (Tekmira Pharmaceuticals Corporation) to develop a vaccine against Ebola. The seed money began at $1.5 million. The value of the deal could grow to an estimated $86 million dollars. [12] In 2013, the Vanderbilt Vaccine Center at Vanderbilt University also received a $4.4 million grant from the US Department of Defense for Ebola vaccine development and other Ebola treatments. [13]
Is Ebola a Threat or a Hoax?
I wish I could definitively tell you whether Ebola is a real threat or a hoax. Based on what I know about the corruption in the pharmaceutical industry, conflicts of interest among political leaders, corporate influence over government agencies, and the agenda of the World Health Organization, I have to say that the truth is buried among a mountain of lies, disinformation, and rapidly changing assumptions.
Should we be concerned about Ebola? Should we be afraid? Should we do whatever we are told by the Centers for Disease Control (CDC), which just happens to hold the patent on this strain of the Ebola virus and all future strains of Ebola? [14]
Even if Ebola is truly a threat, I don’t recommend spending a lot of time worrying about it. I, however, do recommend taking several positive actions.
My recommendations fall into two groups.
First everyone who is concerned about any form of viral or bacterial infection needs to fortify his or her immune system. (See recommendations below.)
The second suggestion involves doing everything you can to avoid taking the Ebola vaccine when it is made available. A strong immune system is the best defense against Ebola. The vaccine will not be a true prevention, and is likely to be filled with toxic substances that will compromise your immune system.
If I am wrong, and the Ebola virus becomes a real threat, then my suggestions regarding building up your immune system will substantially lower your risk of being infected by the Ebola virus. If I am right and there really is little to worry about, then the recommendations will simply give you a stronger immune system, which is a good position to be in regardless of any known or unknown viral threats.
The bottom line is that we do not need to resign control over our health to a government agency or to a pharmaceutical company. We do not need to become helpless victims of an invisible threat if it does exist. We have strong options to lower the risk of contracting this disease and surviving it if we are infected. We have options and we do not need to live in terror of a viral menace!
Does the Conventional Medical System Have a Cure for Ebola?
Scientists from the University of Texas Health Science Center at San Antonio, Texas, indicate that the conventional medical system does not have a curative treatment for Ebola. Even treatments that are being developed by pharmaceutical companies are described as palliative.
Palliative means partial. Thus, the new pharmaceutical drugs for treating cases of Ebola will not be a cure, but will offer partial treatment to those who contract Ebola. Pharmaceutical companies are also working on Ebola vaccines. They hope to begin selling an Ebola vaccine in 2015. [15]
All Ebola Treatments are Experimental
At this point, in October of 2014, we do not have any scientific research which can prove that any specific treatment is effective for curing people who become infected with the currently active strain of Ebola. [16]
At first glance, this might cause some people to fall into a panic about the situation. The good news is that alternative healthcare practitioners have numerous treatments that might be helpful against the Ebola virus. Of course, the herbs, vitamins, and essential oils that could be potentially beneficial, have not been proven as being effective against Ebola. Thus, the pharmaceutical companies and alternative healthcare practitioners are in the same boat. Neither group can claim that they have the cure for Ebola.
At this point, all treatments are experimental. [17] We won’t be able to identify the best treatments until people who actually have the disease are treated for it by conventional and alternative healthcare providers.
It’s Your Immune System that will Cure Ebola
Ultimately, people who contract the disease and survive will need to depend on a strong immune system for survival. The vaccine will not cure a person who already has Ebola. Pharmaceuticals and natural substances will help. But protection from Ebola, if it becomes a real threat, depends on our natural ability to resist viral diseases and the availability of very basic medical care such as proper nutrition and hydration.
USA Today reports Dr. Anthony Faucithe’s analysis of the Ebola situation. He is the longtime director of the U.S. National Institute of Allergy and Infectious Diseases. Dr. Faucithe states:
The most powerful tool against the outbreak is basic medical care. Drugs under development will not be a big part of the solution. They are too early in development for enough doses to be manufactured, even if they are shown to be safe.
The real area of focus, he said, should be setting up medical infrastructure in the affected countries to provide sick people with basic medical support such as replacement fluids and blood. That will have a much bigger effect on health than a few batches of experimental medications.
“That’s the way you help people,” he said. “The idea of ‘What are we going to do with these four treatment courses we have?’ is almost irrelevant of the big picture of the lives that you can save mainly by getting people into proper care.” [18]
Building Up the Immune System
A strong immune system is the best defense for fighting Ebola or any other viral infection. Building a strong immune system involves many factors. It begins with turning away from the standard American high sugar, high carbohydrate, low fat, and highly processed diet. This diet suppresses the immune system.
People who have been weakened by chronic poor nutrition from a standard American style diet, and who are exposed to environmental chemicals, numerous food additives such as preservatives, pesticides and highly processed food ingredients will have a much more difficult time fighting Ebola if they happen to contact the virus.
Fighting Ebola Does not Need to be Complicated
We have been led to believe that our only hope is in the magic formulas and expensive potions of the pharmaceutical industry, but this is quite far from the truth. There are many treatments, which both prevent and cure viral infections. I will discuss a few of the options in the following sections.
Ultraviolet Light from the Sun
Ultraviolet radiation from the sun can be important for Ebola prevention and treatment. The Ebola virus is inactivated when it is exposed to UV radiation. [19] UV light is contained in unfiltered natural sunlight and is available from manmade sources. The Ebola virus can survive in liquid or dried material for a number of days once it leaves the body of the host. [20] This means that hygiene is important for preventing the spread of the virus.
Health Engineers have actually developed a UV robot that can be sent into an area that might contain viruses and/or bacteria and completely disinfect the environment in 2 minutes. This means that high risk environments for Ebola transmission could be easily treated every day if needed. [21]
Vitamin D
Vitamin D is produced in the human body when our skin is exposed to direct sun light. Longtime proponent of vitamin D therapy, Dr. Joseph Mercola, reminds us that vitamin D is essential for healthy immune system functioning. He states:
Regular sun exposure will help optimize your vitamin D, which is crucial for overall robust immune function. Americans in particular may want to take that advice to heart, seeing how most are vitamin D deficient and therefore more open to infections of all kinds. [22]
Vitamin D supplementation is usually needed by people who live in northern climates and are not able to obtain adequate sun exposure.
Vitamin C
Vitamin C destroys viruses or sets them up for destruction by the immune system. Oral doses of high quality vitamin C will prevent viral infections, and intravenous (IV) vitamin C therapy can be used as a powerful cure for active cases of Ebola and other viral infections.
In an article about treating Ebola infection, Dr. Thomas E. Levy, MD, JD recently stated:
To date, not a single virus has been tested that is not inactivated (killed) by a large enough dose of vitamin C (ascorbic acid). Many other antioxidants have similar virucidal effects, but vitamin C appears uniquely to be of greatest potency and clinical efficacy, as its simple chemical structure allows for it to be disseminated throughout the body with little restriction. … Vitamin C is both very potent and optimally bioavailable in accessing any viral infection. [23]
Homeopathic Remedies for Ebola
Many people have found that homeopathic treatments for viral infections have been quite effective.
Dr. Eileen Nauman sites some of the homeopathic remedies that can be useful for treating Ebola. The excerpt from her book states:
Dr. Vickie Menear, MD and homeopath, found that the remedy that most closely fit the symptoms of the 1914 “flu” virus, Crotalus Horridus [rattlesnake venom], also fits the Ebola virus nearly 95% symptom-wise.
During the Spanish influenza epidemic of 1918, eighty percent of the people treated with allopathic drugs died. Eighty percent of the people who took homeopathic remedies, mostly Crotalus Horridus, survived. [24]
Please note: it is not a good idea to try and make your own homeopathic remedy from live Ebola virus. If you wish to use homeopathic treatments, then please consult a qualified homeopathic practitioner.
Silver
The Alliance for Natural Health provides information about Ebola and silver. They state:
Silver … has been used as an antimicrobial for thousands of years. It’s a powerful antibiotic, attacking all kinds of bacteria in a three-pronged attack. … Silver can be used as a method for disinfecting water of both bacteria and viruses. Since disinfecting contaminated environments is the most effective method of halting Ebola’s spread, silver could be a most potent weapon in the battle.
Silver has also showed great promise as an antiviral, in both attacking the virus and in inhibiting transmission. So far, silver has been tested on HIV and herpes. [25]
Red Algae
A substance manufactured in the human body and also found in red algae is useful against Ebola virus. The substance is called mannose-binding lectin. It has a powerful ability to breakdown difficult to destroy viruses such as Ebola. People who have low levels of mannose-binding lectins will have more difficulty destroying the Ebola virus if it enters their bodies. [26]
The most promising form of mannose-binding lectin is a component of the Scytonema varium red algae called Scytovirin. Another anti-viral extract was found from the New Zealand red alga species, Griffithsia sp. This protein is called Griffithsin. [27]
Naturopathic doctor Case Adams explains that red algae can be taken as a supplement against Ebola. He states:
As to whether red algae can be taken in natural form to increase immunity, there is no doubt this is the case. Prior to this antiviral research that has spiraled into biopharm research, red algae had been shown to have antiviral and anticancer effects.
So the most logical answer is “yes” – certainly consuming red algae in supplement form has been found to boost antiviral immunity, and from the available research, blood levels of mannose-binding lectins. This should in turn boost immunity and create a natural method of preventing and even treating viral infections such as Ebola, SARS, HIV and Hepatitis-C. [28]
Melatonin
Researchers who specialize in the study of melatonin have published a report showing that melatonin could be a valuable treatment for treating Ebola infections. Melatonin is most commonly thought of as a hormone that is essential to normal sleep, but it is also a pervasive and powerful antioxidant that protects DNA. The report indicates that melatonin can be used to address severe symptoms of Ebola infection. These include endothelial disruption, disseminated intravascular coagulation (formation of blood clots in the small blood vessels throughout the body), and multiple organ hemorrhage, which commonly occur with an Ebola infection.
They indicated that there are numerous similarities between Ebola virus infection and septic shock. Melatonin has been successfully employed for the treatment of sepsis in many experimental and clinical studies. It could be useful for Ebola as well.
They are encouraging the use of melatonin for Ebola treatment, because there are a limited number of Ebola treatments and a very limited inventory of pharmaceutical drugs for Ebola. Additionally, they are encouraging the use of melatonin, because it has a high safety profile, is readily available and can be orally self-administered. Thus, the use of melatonin would be compatible with situations where there is a large scale outbreak of this infection. [29]
Essential Oils
There are many essential oils that are known to kill viruses. Some of these oils were recognized as effective in previous historical plagues, before they were known as “essential oils,” which is a more modern term. The French perfumers in particular had special plant oils that proved to be effective against many of the historical plagues of the past.
Unfortunately, much of the online knowledge about which essential oils might be effective against Ebola were contained on websites selling these essential oils. Recently, the FDA decided to attack the two largest distributors of essential oils, and force them to remove this information. (See: FDA Targets Essentials Oils: Sees EOs as Threat to New Ebola Drugs?).
The best place to find this information today is probably via books on the subject. If you have the ability to search the Internet in other languages, you might want to try searching in Mandarin Chinese, as the Chinese have a strong herbal and essential oil history.
Pure plant oils are a direct threat to pharmaceutical products, and it appears that the government has used the “Ebola crisis” to finally go after distributors of these essential oils and force them to remove all health claims from the Internet. For an overview on the health benefits of essential oils see my previous article: Using Essential Oils to Cure Disease. We will soon be offering all of my articles on this topic together in an eBook format.
Combining Ebola Treatment Strategies
Dr. Brownstein is a well-known alternative healthcare physician who has done extensive research to help his patients use natural substances to prevent and overcome illnesses. His most recent recommendations, published last week, will help you build up your immune system and respond to the Ebola virus if you encounter it. His recommendations include dosages, which could help you and your healthcare provider use safe alternatives if you need treatment for Ebola virus infection. Dr. Brownstein states:
I say, if you become ill with a viral illness, do the basics to help optimize your immune system. I will show you the four most important items you can use to aid your immune system to fight any illness.
The most important item is vitamin C. Humans are not able to manufacture vitamin C. Either we get enough vitamin C from our diet or the immune system will not function optimally and we will be more prone to becoming ill with various infections, Ebola included. Throughout the medical literature there are many case histories of vitamin C curing viral and other infectious illnesses. Vitamin C activates the immune system so that it can fight any infection.
How much vitamin C should you take? I would suggest taking at least 5,000 mg of vitamin C on a daily basis. If you become ill with any infectious agent, take more as the body’s requirements dramatically increase when it is confronted with an infectious agent.
Intravenous vitamin C should be given to all Ebola patients. Though it has not been studied, I have no doubt that IV vitamin C would be a great benefit to any patient suffering not only from Ebola but from any infectious agent. In my practice, I have used IV vitamin C for over 20 years. Anytime the body is stressed, vitamin C requirements are elevated. IV vitamin C achieves a much higher serum level as compared to oral vitamin C. IV vitamin C should be a standard-of-care treatment for all Ebola patients.
What else can you take to prevent a viral infection? I would suggest taking vitamin A. Vitamin A is integral for the maintenance and functioning of the immune system. In acute viral illnesses, I have found short courses of vitamin A (not beta carotene) very helpful. From 10-100,000 U of vitamin A per day for a few days to a few weeks can stimulate the immune system to fight viral infections.
Vitamin D is also important. Over 80% of patients are deficient in vitamin D. Maintaining adequate vitamin D levels helps lead to a strong immune system. For most patients, I suggest taking 2-6,000 U of vitamin D3 per day. In times of acute illnesses, 50,000 U of vitamin D3 per day for a few days has proven extremely helpful.
Iodine is essential. No virus, bacteria, or parasite has been shown to be resistant to iodine. Iodine levels have fallen over 50% during the last 40 years. Maintaining iodine sufficiency is one of the most important things you can do to help your immune system. For most patients, I have found 12-50 mg/day can supply the body with the correct amount of iodine.
I do not suggest you try taking these large doses of nutrients without seeing a health care provider knowledgeable about natural agents. A competent health care provider can order the appropriate tests and guide you in which therapy is best for you. [30]
Conclusion: Fear May be More Toxic than Ebola
I think there is a high possibility the mainstream media will soon be reporting that the people of the United States are in very serious danger from Ebola, and we must take precautions. We may be told that millions will likely die unless every last American takes the Ebola vaccine. We may be under strong pressure from government leaders, business leaders, religious leaders, and civil authorities to take the vaccine.
According to public health data, it appears that 50% to 90% of people who are infected with Ebola will die even with conventional medical help. As stated earlier, we cannot be sure that the number of deaths that are attributed to Ebola is accurate, thus, the death rate from Ebola could be lower than is claimed.
There are quite a few natural approaches to Ebola prevention and treatment. We do not have to hide in our homes in fear or put on a hazmat suit to go out into public.
It is advised that we clean up our diet, build up our immune system, and send away the fear demons who want us to fall into a hopeless state of despair, so that we will do whatever we are told. Regardless of whether the threat from Ebola materializes in the US, we do not have to become helpless victims. We do not need to fall prey to fear.
This is important, because people are increasingly becoming more and more fearful as news reports fan the flames of an approaching epidemic. When people do not understand a disease such as Ebola, the natural reaction is fear. If people feel there might not be any help for them and their families if they get the disease, the natural reaction is fear. Sustained fear suppresses the immune system. [31] Unrelenting fear can actually contribute to the likelihood of developing Ebola disease if the virus is contacted. In this sense, fear can help spread the disease in a community by lowering the functioning of our immune systems.
A discussion of Ebola or any other threat of epidemic disease would not be complete without mentioning the existence of God and the power of prayer. Those who have a relationship with God will be empowered to enter into His peace and to live under His protection. Those who lack such a relationship may find themselves doing battle with fear, and its friends panic and terror.
If we expect to see Ebola spread through America and we fear for our lives and the lives of our families, then we are putting ourselves under stress. Fear is a tricky fellow. It doesn’t work to tell yourself, “I will not be afraid.” What does work is to prayerfully live in relationship with God who can relieve us of our fear and allow us to live day by day under His care. Those who live in the way of His peace know where they are headed and will be able to trust in Him regardless of what happens.
About the Author
John P. Thomas is a health writer for Health Impact News. He holds a B.A. in Psychology from the University of Michigan, and a Master of Science in Public Health (M.S.P.H.) from the School of Public Health, Department of Health Administration, at the University of North Carolina at Chapel Hill.
References
[1] Gaydos JC1, Top FH Jr, Hodder RA, Russell PK.; “Swine influenza a outbreak, Fort Dix, New Jersey, 1976,” Emerg Infect Dis. 2006 Jan, PMID: 16494712.
[2] “Swine flu ‘debacle’ of 1976 is recalled,” Shari Roan, Los Angeles Times, April 27, 2009, Retrieved 10/10/14. http://articles.latimes.com/2009/apr/27/science/sci-swine-history27
[3] “Reflections on the 1976 Swine Flu Vaccination Program,” David J. Sencer and J. Donald Millar, Emerging Infectious Disease journal – CDC, Volume 12, Number 1—January 2006, Retrieved 10/10/14. http://wwwnc.cdc.gov/eid/article/12/1/05-1007_article
[4] “WHO: Ebola Response Roadmap Situation Report,” World Health Organization, PDF Retrieved 10/10/14. http://apps.who.int/iris/bitstream/10665/136020/1/roadmapsitrep_8Oct2014_eng.pdf?ua=1
[5] “Dept. of Defense Ebola manual: smoking guns,” Jon Rappoport, NoMoreFakeNews.com, October 9, 2014, Retrieved 10/10/2014. http://jonrappoport.wordpress.com/2014/10/09/dept-of-defense-ebola-manual-smoking-guns/
[6] “WHO: Ebola Response Roadmap Situation Report,” World Health Organization, PDF Retrieved 10/10/14. http://apps.who.int/iris/bitstream/10665/136020/1/roadmapsitrep_8Oct2014_eng.pdf?ua=1
[7] “Dept. of Defense Ebola manual: smoking guns,” Jon Rappoport, NoMoreFakeNews.com, October 9, 2014, Retrieved 10/10/2014. http://jonrappoport.wordpress.com/2014/10/09/dept-of-defense-ebola-manual-smoking-guns/
[8] “Ebola,” Jon Rappoport’s Blog, entries about Ebola, NoMoreFakeNews.co. http://jonrappoport.wordpress.com/category/ebola/
[9] “Death doesn’t =someone’s opinion about death,” Jon Rappoport, October 8, 2014, Retrieved 10/10/14. http://jonrappoport.wordpress.com/2014/10/08/death-doesnt-someones-opinion-about-death/
[10] “Grant Gives Alnylam $23M For Anti-Ebola Virus Work,” Randall Osborne, BioWorld, September 29, 2006, Retrieved 10/10/14. http://www.bioworld.com/content/grant-gives-alnylam-23m-anti-ebola-virus-work-0
[11] “Tekmira Nails $140M Defense Contract to Make RNAi Drug for Ebola,” Luke Timmerman, Xconomy, July 15, 2010, Retrieved 10/10/14. http://www.xconomy.com/seattle/2010/07/15/tekmira-nails-140m-defense-contract-to-make-rnai-drug-for-ebola/
[12] “The Monsanto Sponsored Ebola Vaccine Will Kill More People Than the Ebola Itself,” Dave Hodges, The Common Sense Show, August 4, 2014, Retrieved 10/10/14. http://www.thecommonsenseshow.com/2014/08/04/the-monsanto-sponsored-ebola-vaccine-will-kill-more-people-than-the-ebola-itself/
[13] “DoD may send personnel to Africa to help fight Ebola epidemic,” Navy Times, navytimes.com, August 1, 2014, Retrieved 10/14/14. http://www.navytimes.com/article/20140801/NEWS08/308010074/DoD-may-send-personnel-Africa-help-fight-Ebola-epidemic
[14] “The CDC, NIH & Bill Gates Own the Patents On Existing Ebola & Related Vaccines: Mandatory Vaccinations Are Near,” Dave Hodges, The Common Sense Show, September 17, 2014, Retrieved 10/10/14. http://www.thecommonsenseshow.com/2014/09/17/the-cdc-nih-bill-gates-own-the-patents-on-existing-ebola-related-vaccines-mandatory-vaccinations-are-near/
[15] Tan DX1, Reiter RJ, Manchester LC.; “Ebola virus disease: Potential use of melatonin as a treatment,” J Pineal Res. 2014 Sep 27, PMID: 25262626.
[16] IBID.
[17] “Episode 6: Antiviral herbal medicines vs. Ebola and other viral pandemics,” Mike Adams, Health Ranger, – BioDefense.com, Reference to a video teaching session, Retrieved 10/9/14. http://biodefense.com/Pandemic-Preparedness-Episode-06.html
[18] “Fauci: New drugs not the best answer for Ebola,” Karen Weintraub, USA Today, August 6, 2014, Retrieved 10/14/14. http://www.usatoday.com/story/news/nation/2014/08/06/fauci-ebola-drugs/13672605/
[19] “Infectious Disease Index – Ebola virus,” MSDSonline, Retrieved 10/14/14. http://www.msdsonline.com/resources/msds-resources/free-safety-data-sheet-index/ebola-virus.aspx
[20] IBID.
[21] “Ultraviolet light robot kills Ebola in two minutes; why doesn’t every hospital have one of these?” Mike Adams, NaturalNews.com, 10/11/14, 2014, Retrieved 10/14/14. http://www.naturalnews.com/047216_Ebola_contamination_Xenex_ultraviolet_light.html
[22] “Should You Worry About an Ebola Outbreak in the US?” Mercola.com, August 19, 2014, Retrieved 10/14/14. http://articles.mercola.com/sites/articles/archive/2014/08/19/ebola-outbreak.aspx
[23] “Ebola virus can be destroyed naturally without side effects,” Thomas E. Levy, MD, JD, Natural Health 365, August 3, 2014, Retrieved 10/14/14. http://www.naturalhealth365.com/natural_cures/ebola-virus-thomas-levy-1095.html
[24] “CURE FOR EBOLA VIRUS,” Dr. Eileen Nauman, Retrieved 10/14/10. http://www.lightparty.com/Health/EbolaCure.html
[25] “Ebola: WHO Turns To Experimental Drugs, But Not Proven Natural Remedies,” Alliance for Natural Health, September 2, 2014, Retrieved 10/14/14. http://www.anh-usa.org/ebola-who-turns-to-experimental-drugs-but-not-proven-natural-remedies/
[26] “Red Algae Extract Treats Ebola … and HIV, SARS and HCV,” Case Adams, Naturopath, GreenMedInfo, October 9, 2014, Retrieved 10/14/14. http://www.realnatural.org/red-algae-extract-treats-ebola-and-hiv-sars-and-hcv/
[27] IBID.
[28] IBID.
[29] Tan DX1, Reiter RJ, Manchester LC.; “Ebola virus disease: Potential use of melatonin as a treatment,” J Pineal Res. 2014 Sep 27, PMID: 25262626.
[30] “What Can You Do to Prevent/Treat Ebola and Other Viral Infections,” Dr. Brownstein, October 10, 2014, Retrieved 10/14/14. http://blog.drbrownstein.com/what-can-you-do-to-preventtreat-ebola/
[31] “Natural Treatments for Ebola Virus Exist, Research Suggests,” (Page 2), Sayer Ji, GreenMedInfo, August 1, 2014, Retrieved 10/14/14. http://www.greenmedinfo.com/blog/natural-treatments-ebola-virus-exist-research-suggests?page=2